
As of 10 February 2021, 126 confirmed and 56 probable cases of VOC 202012/02 (B.1.351, initially detected in South Africa) have been identified in England. This variant was designated VUI on detection and on review re-designated as VOC 202012/02 (B.1.351) on 24 December 2020.
Genomic profile
The VOC is lineage B1.351 (first sequence detected in South Africa in October 2020; and in the UK in December 2020). The complete mutation profile is shown in Table 4.
| Gene | amino_acid>T | actual_nucleotide |
| S Gene | L18F | 21614C>T |
| D80A* | 21801A>C | |
| D215G* | 22206A>G | |
| R246I | 22299G>T | |
| K417N* | 22813G>T | |
| E484K* | 23012G>A | |
| N501Y* | 23063A>T | |
| A701V* | 23664C>T | |
| 242-244del | ||
| ORF1ab | T265I | 1059C>T |
| K1655N* | 5230G>T | |
| K3353R | 10323A>G | |
| 3675-3677del | 11288_96del | |
| ORF3a | Q57H | 25563G>T |
| S171L | 25904C>T | |
| E Gene | P71L* | 26456C>T |
| N Gene | T205I* | 28887C>T |
| CONFIRMED | All lineage defining non-synonymous changes called as alternate base excluding those in red text in Table 4a |
| PROBABLE | At least 4 lineage defining non-synonymous changes called as alternate base and all other positions either N or mixed base OR at least 5 of the 9 non-synonymous changes indicated by * in the Table 4a |
| LOW_QC | Fewer than 4 lineage defining non-synonymous changes called as alternate base and all other positions either N or mixed base |
Biological profile
This variant has 9 mutations associated with transmissibility and antigenic change, of which E484K and N501Y are most significant. The significance of E484K has been described previously in this briefing. Variants with the combined N501Y and E484K substitutions have been shown to have enhanced ACE2 receptor binding.
Escape from natural immunity
Multiple studies with pseudovirus and live virus neutralization assays indicate a significant loss of antibody binding and neutralization to B.1.351, both with convalescent, as well vaccinederived polyclonal antisera.
Epidemiological profile
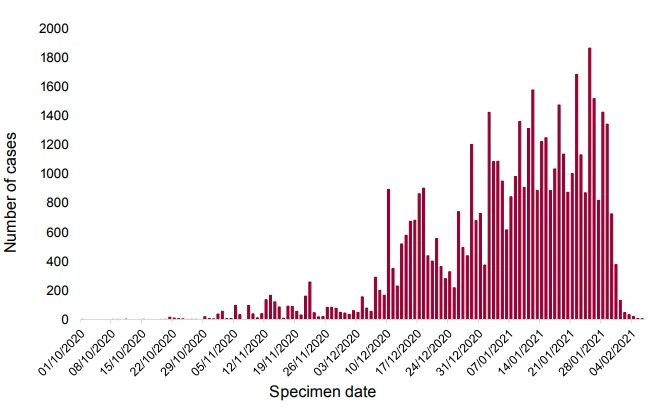
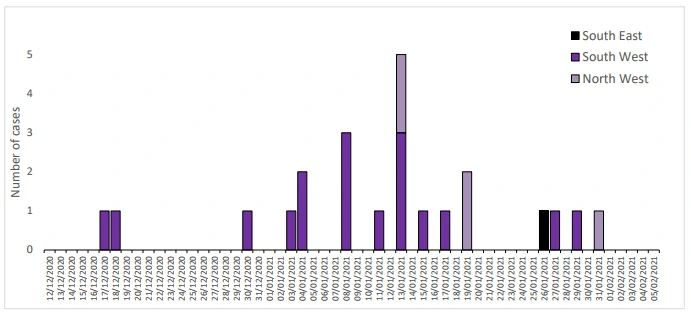
B1.351 is dispersed across the UK in low numbers. Confirmed cases are those identified by whole genome sequencing; probable cases are COVID-19 cases without sequencing, but who are contacts of confirmed cases. As of 10 February 2021, there are 126 confirmed cases of B.351.1 and 56 probable cases. For 18 cases, no travel link has been established indicating within country transmission. Identification of unlinked cases through Pillar 2 is limited by sequencing coverage and lag and cases are likely to be an underestimate.
Figure 4. Epidemic curve for confirmed VOC 202012/02 (B.1.351) cases by specimen date, 10 December 2020 to 10 February 2021 (7 cases are omitted without specimen date)Percent confirmed SGTF for most recent days annotated.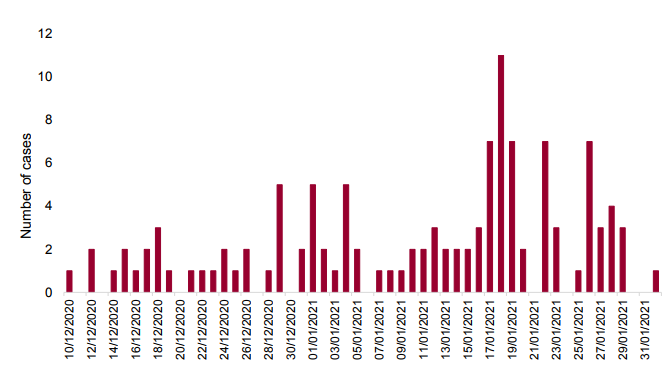
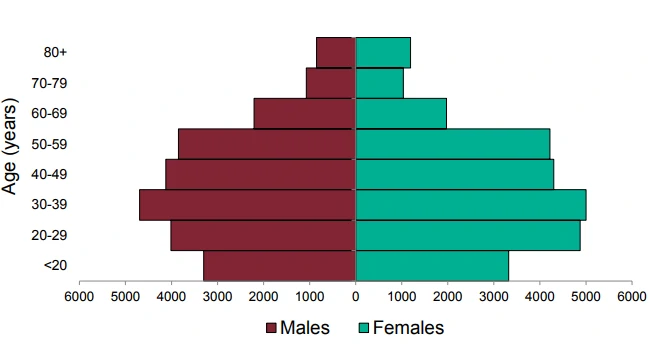
Figure 5. Age sex pyramid of VOC 202012/02 (B.1.351) confirmed cases, 10 December 2020 to 10 February 2021 (3 cases are omitted without age sex data)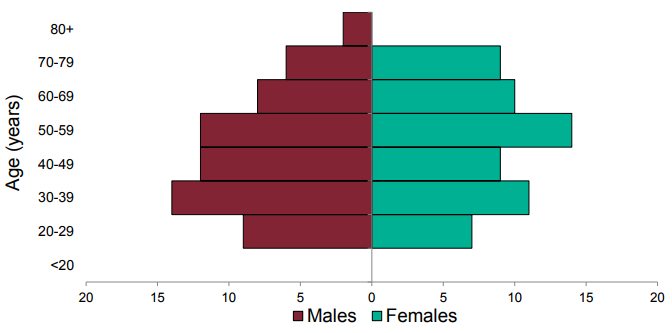
| PHE Centre | VOC 202012/02 (B.1.351) | All sequenced | ||
| n | % | n | % | |
| East Midlands | 3 | 2.4 | 6 808 | 5.2 |
| East of England | 26 | 20.6 | 13 445 | 10.3 |
| London | 31 | 24.6 | 29 350 | 22.5 |
| North East | 2 | 1.6 | 8 194 | 6.3 |
| North West | 14 | 11.1 | 28 099 | 21.5 |
| South East | 30 | 23.8 | 14 630 | 11.2 |
| South West | 4 | 3.2 | 5 126 | 3.9 |
| West Midlands | 11 | 8.7 | 11 300 | 8.6 |
| Yorkshire and Humber | 5 | 4.0 | 13 657 | 10.5 |
| TBC | 0 | 0.0 | 77 | 0.1 |
| Total | 126 | 130,686 | ||
Community prevalence studies
REACT study: Altogether 4 VOC 202012/02 (B.1.351) genomes were identified. SARS-COV-2 was detected in 2,282 of 167,642 samples during 6 to 22 January 2021. Of these, samples with CT values of 34 or less had sequencing attempted; 659 have available sequences, of which 4/659 are VOC 202012/02 (B.1.351) from East of England (2), London (1) and South East (1). All have sample dates between 7 to 11 January 2021. (Link to Study protocol.)
Office for National Statistics Survey
The ONS survey identified 2 cases of VOC 202012/02 (B.1.351) in samples from December 2020. A total of 1,816 sequences were available for 1 December 2020 to 20 January 2021.
Deaths
1 death (within 28 days) of 126 confirmed cases with data has been reported in patients with VOC 202012/02 (B.1.351) as of 10 February 2021.
Cases in individuals who have been vaccinated
Vaccination data is being assessed.
International Epidemiology
As of 10 February 2021 there are 40 countries (including the UK) that have reported cases of this variant globally.
As of 10 February 2021 the epidemiological profile in South Africa is as follows:
• The case incidence is continuing to decrease. Currently, the reported weekly incidence is 34.2 per 100,000 population. Weekly test positivity has also been decreasing with current test positivity of 9.7% (testing rates had increased over the period from around 2 per 1,000 population to over 6 per 1,000 population, although have declined slightly over the last 2 weeks to 3.5 per 1,000 population).
• The fatality rate is decreasing (the weekly fatality rate is 3.2 per 100,000 population).
• The number of patients in hospital and ICU has also reduced slightly.
Currently, 1,839 COVID-19 patients are in ICU and 11,618 are in hospital.
GISAID (gisaid.org) includes data on sequences available internationally. As of the 12 February 2021 1,130 cases of VOC 202012/02 (B.1.351) are listed (Australia 17, Austria 3, Bangladesh 1, Belgium 59, Botswana 35, Canada 1, Denmark 7, Dominican Republic of the Congo 1, Finland 2, France 39, Germany 8, Ireland 10, Israel 7, Japan 5, Kenya 6, Luxembourg 2, Mayotte 23, Mozambique 42, Netherlands 31, New Zealand 7, Norway 1, Panama 1, Portugal 1, South Africa 749, South Korea 1, Spain 2, Sweden 1, Switzerland 23, Turkey 2, UAE 5, USA 7, Zambia 31).
| Week beginning | Percentage VOC of all Δ69-70 | Number of pillar 2 Δ69-70 sequences |
| 2020-10-12 | 3% | 116 |
| 2020-10-19 | 15% | 220 |
| 2020-10-26 | 29% | 156 |
| 2020-11-02 | 64% | 399 |
| 2020-11-09 | 81% | 711 |
| 2020-11-16 | 88% | 805 |
| 2020-11-23 | 93% | 390 |
| 2020-11-30 | 95% | 433 |
| 2020-12-07 | 98% | 2,712 |
| 2020-12-14 | 99% | 4,300 |
| 2020-12-21 | 99% | 2,407 |
| 2020-12-28 | 99.7% | 5,070 |
| 2021-01-04 | 99.7% | 5,621 |
| 2021-01-11 | 99.9% | 7,473 |
| 2021-01-18 | 99.8% | 6,088 |
| 2021-01-25 | 100% | 1,222 |
| Region | Percentage VOC 202012/01 (B.1.1.7) of all Δ69-70 | Number of Pillar 2 Δ69-70 1 to 31 January 2021 |
| East Midlands | 99.9% | 669 |
| East of England | 99.9% | 2095 |
| London | 99.8% | 4819 |
| North East | 100% | 871 |
| North West | 99.8% | 6615 |
| South East | 99.6% | 2875 |
| South West | 99.9% | 671 |
| West Midlands | 99.6% | 2100 |
| Yorkshire and the Humber | 99.6% | 1283 |
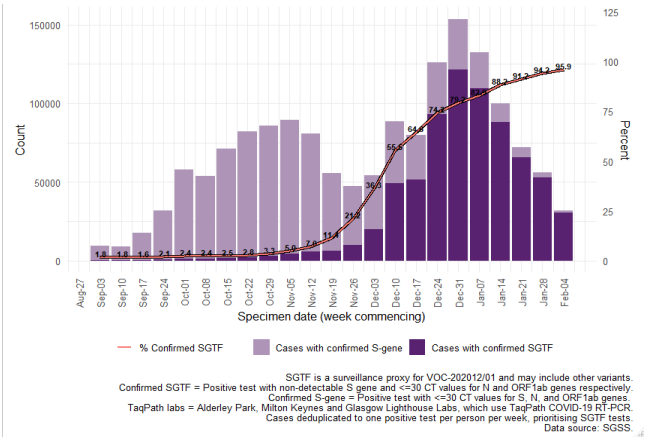 Figure 7. Weekly number and proportion of England Pillar 2 COVID-19 cases with SGTF among those tested with the TaqPath assay and with S gene detection results, by region of residence (3 September 2020 to 10 February 2021)
Figure 7. Weekly number and proportion of England Pillar 2 COVID-19 cases with SGTF among those tested with the TaqPath assay and with S gene detection results, by region of residence (3 September 2020 to 10 February 2021)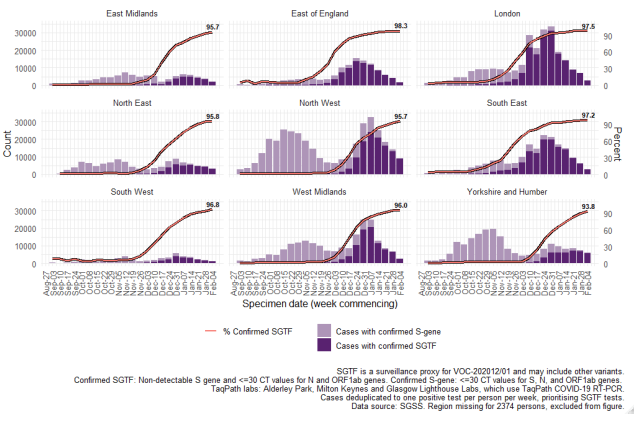 Data on coverage of TaqPath laboratories testing and numbers/proportions of cases with SGTF are shared daily with Local Authorities (Sunday to Friday) on the COVID-19 PHE Local Authorities Report Store (Sharepoint).
Data on coverage of TaqPath laboratories testing and numbers/proportions of cases with SGTF are shared daily with Local Authorities (Sunday to Friday) on the COVID-19 PHE Local Authorities Report Store (Sharepoint).